BOOK OF THE MONTH

Nasser My Husband
By: Tahia Gamal Abdel Nasser
Category: Biography
Tahia Gamal Abdel Nasser and Tahia Khaled Abdel Nasser American University in Cairo Press Arabic version by Dar Shorouk Gamal Abdel Nasser, architect of Egypt's 1952 Revolution,...
TRENDING BOOKS





Recent from E-Zine
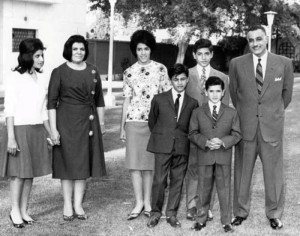
Mona Abdel Nasser Speaks
By: Ibrahim Khalil on: Friday 24 July 2026 - Genre: Biography
الزعيم جمال عبد الناصر حسين خليل سلطان المري من مواليد 15 يناير عام 1918 في منزل والده رقم 12 شارع قنوات بحي باكوس في الإسكندرية وهو من أسرة صعيدية عربية قحطانية حيث ولد والده في قرية بني مر في محافظة...

I am a Watermelon Seller
By: Omar Hammash on: Wednesday 22 July 2026 - Genre: Stories
مثل كائنٍ قديم، أتتبع زحف الليل على الخيمة. ثقيلاً يمرّ، كأنه فيل جثم ونسي نفسه. وهذا الحرّ يسقطه سقف القماش الساخن. ولي عينان أعرف أنهما موجودتان، وساقان سقطتا، أثقل من خرسانة كالتي أسقطها القصف في ب...

Egyptian cinema: between adaptive and rebellious creativity
By: Mona Helmy on: Monday 20 July 2026 - Genre: Arts and Entertainment
كيف وصلت السينما المصرية ، الى هذا الحال ، الذى لا يرضى صُناع الفن السابع ، والملايين من عُشاق الشاشة الفضية ؟. كمصريات ومصريين ،...

Messi: Minimal Effort, Maximum Return
By: Rabab Kamal on: Sunday 19 July 2026 - Genre: Sports
البيانات الرسمية الصادرة عن الاتحاد الدولي لكرة القدم (الفيفا ) للإحصائيات الرياضية تكشف أن ليونيل ميسي يسير ( لا يجري ) ما يقارب 83% من وقت المباراة ، وهي نسبة تم توثيقها بدقة عبر تقنيات التتبع البصر...

The Beloved Villain in Cinema and Theater
By: Hayel Ali Al-Mathabi on: Saturday 18 July 2026 - Genre: Arts and Entertainment
في حكايات "ألف ليلة وليلة"، تبرز شخصية "علي الزئبق" لـتؤدي وظيفة الشرير المحبوب لدى الجماهير، ويسري هذا التقليد نفسه على شخصية "روبن هود" في الغرب، لتؤدي الوظيفة ذاتها عل...

The Cost of War and the Value of Peace
By: Mouloud Benzadi on: Friday 17 July 2026 - Genre: Opinion
Among the most powerful quotes left by Walter Scott, the Scottish novelist and poet, one remains relevant nearly two centuries after his death: “War is the only game in which both sides lose....

The Inverted Red Triangle
By: Ben Younis Majen on: Wednesday 15 July 2026 - Genre: Poetry
من رحم الالم يولد الأمل موجه الى الاسفل لقنص الحشرات الضارة انه السهم القاتل الذي كان يلاحق طرائده أينما ظهرت بين الأنقاض والأطلال و الحفر من كوة في الجدار تطل بند...

بيتنا الطيني
By: Khira Jalil on: Thursday 9 July 2026 - Genre: Poetry
في بيتنا الطين ي في بيتنا الطيني ضفرت جدائل حلم من طينة الصبار ما كان سكناً بل قصرا بمائات الابواب مشرعة حد الخطيئةِ وموصودة حد النصيحة. من يجرؤ على اقتح...
Upcoming Events

Artificial Intelligence: Ethical Concerns
May 23, 2026
This presentation took place on May 23rd, 2026. Yo...

?Who is the intellectual? And what is the role of the cultural reformer in societies
April 13 - 15, 2026
محاضرة يلقيها الفيلسوف والمفكر الإسلامي م.محم...

Mnemonic the Play, A Presentation and Discussion
January 24, 2026
This presentation and discussion of Mnemonic the P...

Sufism between deconstruction and theory
September 11, 2025
A religious and scientific dialogue on Sufism, i...